Welcome back to our Colpo Corner, where we explore various aspects of colposcopy. In this edition Mary Rubin, PhD, WHNP-BC, FAANP shares her advice on performing colposcopy during pregnancy based on her 35 years of experience working in colposcopy.
Performing colposcopy during pregnancy can be daunting for many clinicians. However, it is very safe as long as you follow the appropriate guidelines. The main issue to remember is that in essence there are two patients instead of one – both the mother and her unborn baby.
When to perform colposcopy in pregnancy
The purpose of performing colposcopy in pregnancy is to rule out the presence of cancer (frank invasion). The American Society for Colposcopy and Cervical Pathology (ASCCP) states that 3-6% of Pap tests performed during pregnancy have abnormal results and that cancer occurs in 1:2000-2200 pregnancies.
It is essential that nothing be inserted deep into the endocervical canal as you could disrupt the pregnancy by instrumenting the canal. For some women, the cervix is lower lying during pregnancy, and at times even the placenta could lie within the womb against the cervix. Inserting anything could even perforate the amniotic sac if the cervix is over dilated. (see Case Study 1).
It is vital that nothing be placed deep within the birth canal, and clinicians should never perform endocervical curettage on a pregnant patient.
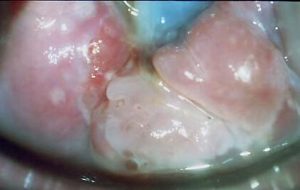
CASE STUDY 1
Dilating cervix with a visible bag of water. Posterior acetowhite High-Grade lesion.
Physiological changes
Hormonal influence during pregnancy leads to various physiological changes. The ease of performing colposcopy varies greatly depending on how far the pregnancy has progressed. One sees less physiological changes to the cervix during the first trimester. Significant changes usually start in the second trimester as the baby gains weight and presses on the cervix.
Lax vaginal walls
The walls of the vagina often soften becoming lax and less elastic, which can impair the clinician’s ability to visualize the cervix. Even after inserting a speculum, the walls of the vagina may ‘droop’ down through the gaps between the blades of the speculum. Using a vaginal retractor in conjunction with the speculum can resolve this issue. With the speculum in place, insert the vaginal retractor that its blades fit between the blades of the speculum, holding all the walls of the vagina in place.
The challenge of clear visualization is compounded as the cervix increases to up to ten times in size during pregnancy, leaving the clinician with a larger cervix to visualize and a less elastic vagina.
If not yet possible to obtain a clear view of the transformation zone, with an adequate amount of the endocervical canal and squamocolumnar junction may require using an endocervical speculum. Use with caution so as not to disrupt the amniotic sac or another impact on the growing baby, as discussed above. Copious mucus from the abundant glandular tissue add to difficulties in visualization. (See Case Study 2)
CASE STUDY 2
Abundant glandular epithelium

Condoms can simplify colposcopy in pregnancy
It can be very taxing for both the clinician and the patient to manage a procedure that may require the insertion of three separate instruments into the vagina. Some experienced colposcopists use an innovative method to do away with the vaginal retractor. Placing a condom over the speculum before insertion and cutting off the tip of the condom so that it forms a sheath around the speculum to hold the lax walls of the vagina in place with minimal invasion to the patient while the cervix remains clearly visible.
Frequently, when performing colposcopy in pregnancy, I would recommend placing a condom sheath on the speculum as a matter of course. (This method can also apply to patients with a large body habitus in general colposcopy cases.)
Risks of bleeding during biopsy
The genital tract increases in vascularity as pregnancy progresses. This poses complications for biopsy collection as the area will likely bleed more, and it is harder to stop bleeding.
This significantly impacts the biopsy procedure. While screening a non-pregnant patient, one might err on the side of taking more biopsies to ensure the evaluation of any and all problematic areas. During pregnancy, one must take as few biopsies as possible to rule out the presence of cancer. A clinician must judiciously select the most abnormal looking tissue to biopsy as heavy bleeding can easily result.
Treatment options for abnormal findings
If colposcopy/biopsy confirms that a patient has precancerous lesions, then it is sufficient to monitor them during their pregnancy for reevaluation and schedule treatment during postpartum. Ideally, the patient should return at 8 weeks postpartum for reevaluation.
It is not possible to perform any sort of treatment until at least 6 weeks postpartum, as the cervical tissues are still going through reparative changes following birth.
8 weeks postpartum represents the ideal treatment time. However, some insurance will only cover patients until 6 weeks postpartum requiring earlier treatment if necessary.
While rare, the development of fully cancerous lesions during pregnancy does happen. If visualization suggests the possibility of cancerous lesions, then a physician should perform either a wedge resection of the abnormal area or a full cone biopsy. Should cancer be confirmed, then referral to a gynecological oncologist for a comprehensive assessment is required as to whether it is safe for the women to carry the pregnancy to term. Doctors may need to induce early labor once the pregnancy is viable. At this point, the mother’s personal and religious beliefs play a significant role. If the woman needs immediate treatment including radiotherapy, a termination of the pregnancy would be advised.
Colposcopy in pregnancy requires the clinician to balance the physical/medical needs of the patient with her emotional/psychological needs. The procedure itself requires some adjustments from standard colposcopy practice while constantly reassuring the patient of her and her baby’s her wellbeing.
Check out other recent articles in our Colpo Corner series:
- DES daughters: Understanding DES (Diethylstilbestrol) and its clinical implications
- Explaining colposcopy to patients: A multi-disciplinary perspective
- 8 ways to make a colposcopy less scary for your patients
About the collaborating author:




